This article summarises key learning points from the 2026 More Than Medics x BiteLabs HealthTech Foundations Scholarship. A four-week programme that gave 48 UK medical students a credible, structured entry point into digital health – and proof that clinical curiosity is a real competitive advantage.
Medical students are routinely told they will one day lead teams, advocate for patients, and navigate complexity under pressure. Less often are they told that those exact skills translate directly into building healthcare technology. That gap, between clinical training and the innovation ecosystem, is precisely what the More Than Medics x BiteLabs HealthTech Foundations Scholarship was designed to close.
Run across four weeks from January to February 2026, the scholarship brought together 48 medical students for a free, fully online programme covering digital health fundamentals, product thinking, the healthtech ecosystem, and career pathways into the sector. No prior technical experience was required. What participants brought with them mattered far more: genuine curiosity, a tolerance for uncertainty, and familiarity with the clinical problems that digital health exists to solve.
The results spoke clearly. Scholar self-rated confidence in healthtech climbed from 2.9 to 4.7 out of 5. Competency scores rose from 3 to 4.5 out of 5. 95% of scholars finished feeling equipped to engage meaningfully with the field.
Top performers in the capstone project were awarded Distinction Scholar status, a formal Distinction certificate, a one-to-one mentorship session with BiteLabs, an invitation to BiteLabs Demo Day, and a public LinkedIn feature. Outstanding contributions throughout the programme were also recognised through the Award of Merit. These are real credentials, worth building towards.
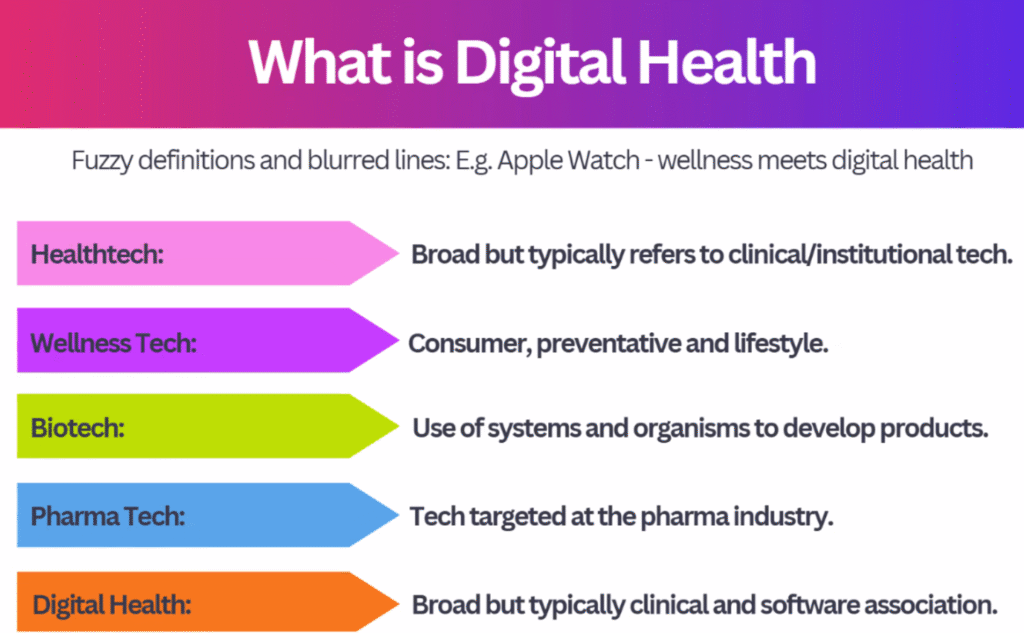
🤔Week 1: What is Digital Health?
The opening session, led by Dr. Leslie Dickson-Tetteh, unpacked the concepts that underpin the field: how digital health is defined, what interoperability means in practice, and the patterns that cause promising projects to stall. A fireside chat with Dr. Jing Ouyang, Dr. Onayomi Rosenior-Patten, and Lucy Marples gave scholars an honest account of what building a career at this intersection actually looks like.
The group exercise set the tone for the whole programme. Given 15 minutes and a real NHS problem, teams had to propose a digital solution and defend it. Speed forced prioritisation. One group tackled discharge bottlenecks caused by fragmented multidisciplinary coordination; another looked at how digital tools might improve patient flow. The hardest part was not generating ideas but being ruthless about which ones were genuinely useful rather than impressive.
The recurring message: solutions that do not integrate naturally into existing clinical workflows face enormous adoption barriers, regardless of technical sophistication. Patient-centred design is not a buzzword – it is a practical filter. The relevant questions are concrete: who is this for, what friction does it remove, and how would you know it helped?
Doable next step: Over your next placement, keep a note of specific friction points. Not vague inefficiency, but precise moments where a workflow broke down, who was affected, and what a better version might look like. That discipline of observation is where the most valuable healthtech problems get found.
💡Week 2: From Idea to Solution
Week 2 brought Dr. Vish Menon, Senior Clinical Lead at Accurx – a platform used by 98% of GP practices and 68% of NHS trusts, and through which 30 million COVID vaccines were booked. He explained how Accurx got there, and the answer was not what most people expect.
The team spent six months simply observing workflows at GP practices before building anything. Watching every task, every role, every handover. Their conclusion: healthcare is fundamentally a communication industry. When COVID created an urgent need for GP consultations to move online via video calls, Accurx deployed a video consultation feature across a single weekend. Adoption jumped from roughly 30% to 95% across the NHS within days – made possible by six months of prior understanding, not speed alone.
Scholars also worked through the Stanford Biodesign framework, Jobs-To-Be-Done statements, and agile versus waterfall development. The AI content was equally pointed: models are only as good as their training data, and poorly representative data does not improve on existing healthcare inequalities – it scales them.
Two phrases from this session stayed with scholars throughout the rest of the programme:
💡”useful beats impressive” and “narrow beats magical.”
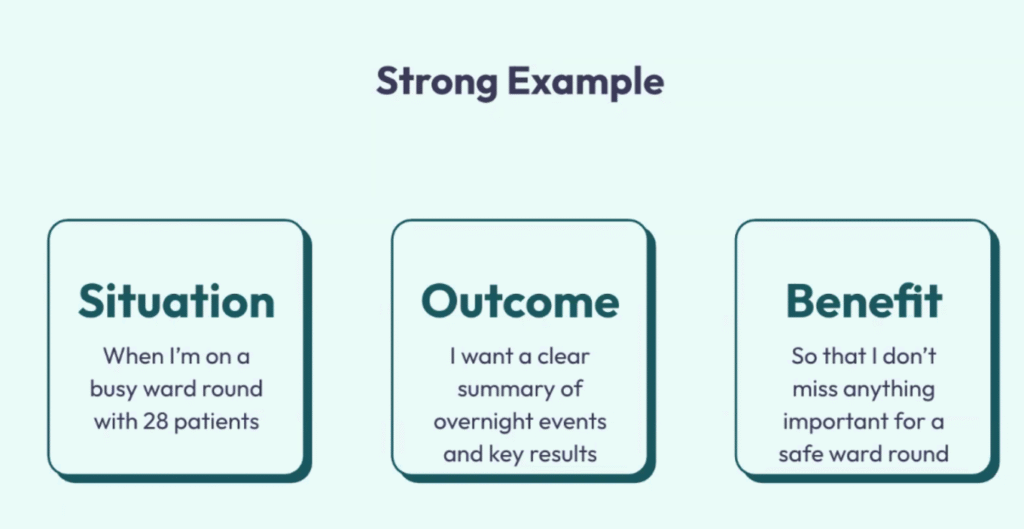
Doable next step: Write a JTBD statement for a clinical problem you have observed. The format is: “When [situation], I want to [motivation], so I can [outcome].” Write three versions. The process of refining them is the skill.
🌐Week 3: The HealthTech Ecosystem
Dr. Michael Trueman, co-founder and CEO of Advoca Health, led a session focused on what it takes to move a healthtech idea from concept to implementation. A regulatory panel featuring Emma Dyson, Tom Micklewright, and Jonathan Gregory addressed clinical safety standards and their practical implications for product development.
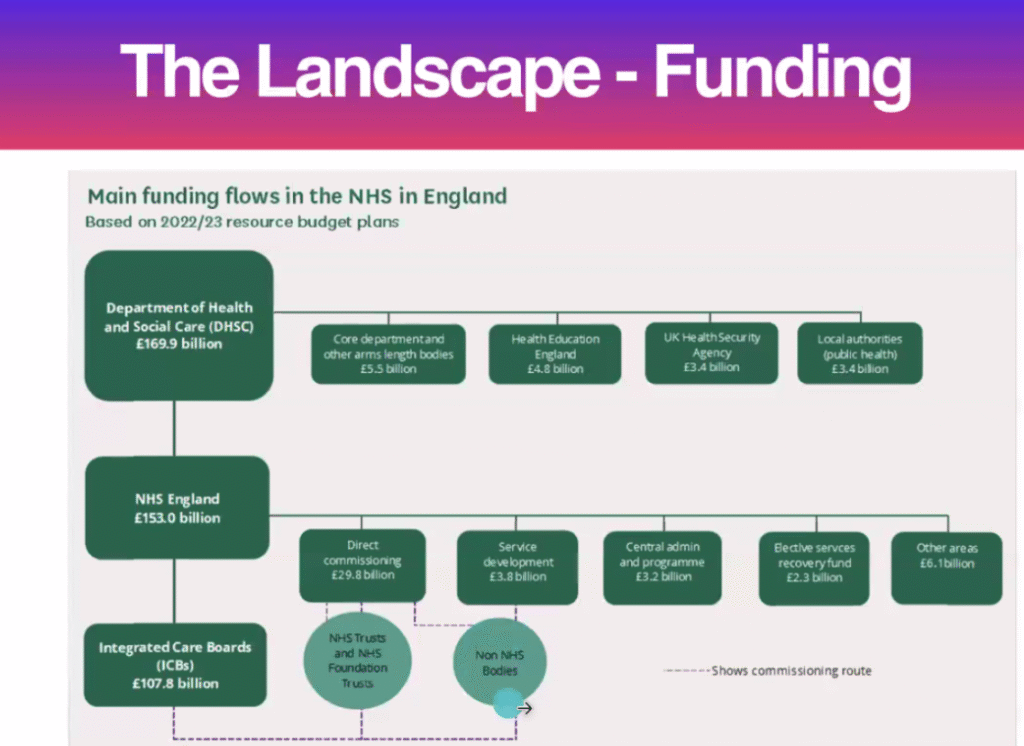
The session mapped the NHS as a layered system of commissioners, providers, budget holders, and regulators – each with different incentives and timelines. Case studies including Patchwork Health, Concentric, and Behold.ai illustrated how structural features of the system create specific barriers, and why products that strengthen existing workflows tend to gain traction more reliably than those positioned as disruptors.
The key lessons were blunt. Safety and regulatory thinking belong at the start of a project, not appended when procurement teams start asking questions. Budget holders need to be engaged early in any commercial conversation. Untapped opportunity in healthtech is often found at the edges of the system – pharmacy, optometry, dentistry – rather than in areas already receiving heavy investment like GP care and radiology.
Doable next step: Research one of the programme’s case studies. Read about how it started, who its early customers were, and which parts of the NHS ecosystem it had to navigate. The patterns are instructive and transfer across contexts.
📈Week 4: Career Pathways and Next Steps in Digital Health
The final week, anchored by Dr. Bharadwaj Chada, addressed the practical question of how clinicians build meaningful careers in digital health. Dr. Brogan Rudge and Dr. Jonathan Andrews introduced scholars to “shiny object syndrome” – the gap between how an opportunity looks from the outside and whether it genuinely aligns with your motivations. Jason Spinney followed with a grounded session on LinkedIn, CV construction, and healthtech hiring, with a clear message: demonstrated curiosity matters more to employers in this space than transferable skills listed on paper.
The week culminated in Demo Day, with capstone pitches judged by Dr. Louise Rix and Olu Arisekola. The range of ideas was striking. Group 11 won Distinction Scholar status with their product, Digital Dosset, an app addressing medication adherence in primary care. The Gut Guide tackled IBD symptom management for young people transitioning from paediatric to adult services. WoundWatch proposed an AI-powered monitoring system for surgical site infections. All three emerged from four weeks of work, with no prior product development background required.
The capstone structure forced scholars to hold together problem definition, stakeholder mapping, clinical relevance, and commercial logic – then communicate it in four minutes. Several scholars who had never pitched before found it the most stretching part of the programme, and the feedback from judges was where some of the most useful learning happened.
Doable next step: Write a one-paragraph version of a capstone idea or clinical problem you care about. Not a deck – one paragraph, as if explaining it to a peer. Where it becomes vague is where the thinking still needs work.
🚀Looking Ahead
This scholarship does not try to convert medical students into product managers. What it does is give future clinicians the vocabulary, frameworks, and network to engage with digital health as active participants rather than passive recipients. The curiosity they already have, sharpened by clinical experience, turns out to be exactly what the field needs.
Applications for the next cohort will be announced on the more than medics newsletter in due course. The programme is online, and designed to sit alongside existing commitments. The only real prerequisite is a genuine interest in how healthcare could work better.
Start there. See where it leads.
💭A note from a Distinction Scholar
Winning Distinction Scholar status with my capstone project was genuinely rewarding, but looking back, some of the most valuable parts of the programme had nothing to do with the formal content. Pay real attention to the people around you. The scholars you discuss problems with in breakout rooms, the teammates you work through tasks with, and the peers who push back on your thinking often teach you things no session can replicate.
Healthtech is a fundamentally collaborative field, and how you show up in a team – your openness to other perspectives, your willingness to build on someone else’s idea rather than default to your own, your attitude when a plan needs to change – matters as much as what you know. Go into your capstone group with genuine investment in everyone’s contribution, not just the final pitch. The relationships you build across four weeks, and the version of yourself you bring to those interactions, will follow you far beyond Demo Day.
Thanks for reading. If you have any comments or suggestions, please feel free to share them below and we’ll get back to you as soon as we can!




